Why TR-MRA?
Contrast-enhanced TR-MRA offers quasi-real time vascular imaging with sufficiently high temporal resolution to assess contrast flow dynamics in arteries and veins using only a small contrast dose.
Advantages of TR-MRA include short acquisition time,
high-temporal resolution,
reduced motion artifacts,
and the ability to selectively visualize arteries and veins without the hassle and complexity of estimating contrast bolus arrival times.
High temporal resolution is especially valuable for imaging arteries in anatomical areas with rapid venous return,
including the neck,
pulmonary circulation,
kidneys,
and high flow vascular lesions such as some arteriovenous malformations.
High temporal resolution is also useful to image vascular beds with staggered enhancement,
such as the true and false lumina in arterial dissection,
vascular stenosis,
and vascular occlusion with collateral formation.
The high temporal resolution of TR-MRA is achieved at the expense of decreased spatial resolution compared with single-phase contrast-enhanced bolus-chase 3D MRA.
As a result,
assessment of small vessels and depiction of some vascular pathologies could be compromised.
Therefore,
care must be taken to ensure an appropriate tradeoff between temporal and spatial resolution for a particular clinical application.
TR-MRA provides similar diagnostic information to DSA,
but is noninvasive and avoids exposure to ionizing radiation and nephrotoxic and allergenic iodinated contrast material.
Consequently,
TR-MRA is beginning to supplant DSA for many clinical applications.
All TR-MRA methods trace their origins to the keyhole imaging method.
Keyhole imaging was developed in the 1990's and was used primarily for dynamic contrast-enhanced 3D MRA of vascular lesions and tumors.
The central phase-encoding lines were sampled repeatedly using a rectilinear or Cartesian k-space grid after contrast injection,
whereas the peripheral lines were sampled sporadically and less frequently.
View-sharing was then used to produce a set of full-resolution images from several k-space data sets.
K-space undersampling with parallel imaging can further decrease the data acquisition time.
Several modern ultrafast TR-MRA techniques use 2D or 3D radial k-space sampling schemes with aggressive undersampling and view sharing.
The most extreme example of undersampling is 3D MRA with compressed sensing.
This promising ultramodern technique dramatically reduces the acquisition time by exploiting the sparsity of MRA k-space data.
The sparse data are then fed into a mathematically complex iterative image reconstruction algorithm.
3D MRA with compressed sensing offers very high temporal resolution without view sharing.
Technical aspects of TR-MRA:
The exact imaging parameters for a contrast-enhanced TR-MRA will vary depending on scanner hardware and software,
the required anatomic coverage (FOV),
the dimensions of the smallest clinically relevant vessel or other structure,
and the flow characteristics of the vascular bed or pathologic entity.
The core of most TR-MRA methods is a heavily T1-weighted 3D spoiled gradient-recalled echo (GRE) pulse sequence with a low flip angle and a very short repetition time (TR,
typically 1-2 ms) and echo time (TE,
typically <1 ms).
Acquisition times are further reduced by using aggressive k-space undersampling techniques,
such as read-conjugate and phase-conjugate symmetry as well as parallel imaging with acceleration factors of 2-6,
depending on the surface coil geometry and magnetic field strength.
The temporal resolution of TR-MRA typically ranges from 1-5 s/frame.
The temporal footprint of each frame depends on the temporal resolution per frame and the number of frames that contributed data to each image.
Total scan time ( = # measurements x temporal resolution) is usually 30-40 seconds,
but may vary depending on the particular clinical application.
After zero-filling in the slice direction (and sometimes also in the phase direction),
the interpolated voxel dimensions range from 0.8 × 0.9 × 0.9 to 1.1 × 1.4 × 1.5 mm.
TR-MRA presents an inherent tradeoff between spatial and temporal resolution.
Several novel strategies based on keyhole imaging have been developed to optimize these competing demands.
Recall that the center of k-space contains information about image contrast,
whereas the periphery of k-space defines edges and fine details.
In one vendor’s implementation of TR-MRA (TWIST,
Siemens),
k-space is fully sampled in the center (C) and undersampled at the periphery (P) using a quasi-random sampling scheme.
The user selects the size of the central k-space region (C,
typically 15-30%),
the central k-space refresh rate (in frames per second),
the undersampling fraction of the peripheral region (P,
typically 20-30%),
and the total number of frames to be acquired (depends on anticipated circulation time).
Sampling more points in the periphery requires additional imaging time,
which adversely impacts temporal resolution.
The parameters having the greatest impact on imaging speed include the sizes of regions C and P,
the degree of undersampling of P,
and the parallel imaging acceleration factor.
These parameters must be tailored for each case based on the clinical question,
the desired anatomic coverage,
and the required temporal and spatial resolution.
Time-resolved MRA techniques balance the competing demands of temporal and spatial using a method known as view-sharing.
The details of these methods vary by vendor,
but the common thread is that a “complete” full resolution image is created at a particular time point by stitching together the current central k-space data (C) and portions of several undersampled peripheral k-space datasets (P) from nearby time points.
During passage of the contrast bolus,
C is sampled much more frequently than P.
Several vendor-specific keyhole imaging strategies are detailed below:
- Siemens TWIST ("Time-resolved angiography With Stochastic Trajectories") divides k-space into two regions,
but samples them alternately using a semi-randomized method.
The peripheral region is sparsely sampled at each time point,
although is eventually covered over several cycles.
- GE TRICKS ("Time-Resolved Imaging of Contrast KineticS") divides k-space into four concentric regions (A-D,
from inner to outer),
sampling them in the order --A-B-A-C-A-D--A-B-A-C-A-D--
- Philips 4D-TRAK ("4D Time-Resolved Angiography using Keyhole") is a centric version of the classic keyhole method,
where k-space is divided into a central and peripheral oval regions.
The central region is sampled much more frequently than the peripheral region.
- Toshiba uses Freeze Frame.
- Hitachi uses TRAQ ("Time-Resolved AcQuisition")
Most TR-MRA sequences begin by acquiring a full-resolution image set prior to arrival of the contrast bolus.
These image will be used as the mask to make post-contrast subtracted raw data and MIP images with improved vascular conspicuity.
The gadolinium-based contrast agent is injected as a tight bolus at 2-3 cc /sec and followed by saline chaser.
A contrast timing bolus is not required and should not be performed due to the risk of contrast contamination of the mask images.
TR-MRA generates sequential volumetric image sets at 1 to 5 second intervals for up to several minutes after injection of contrast.
Subtracted MIP reconstructions from the sequential volumetric image data can be played as a cine loop to give the appearance of real time fluoroscopic imaging.
Differences between TR-MRA and conventional contrast-enhanced MRA
While most bolus chase contrast-enhanced 3D MRA techniques obtain images at only one or two time points after contrast injection,
TR-MRA obtain a series of images depicting passage of the contrast bolus.
A typical TR-MRA study may contain 20 or more time frames obtained at rates as rapid as 1-2 frames per second.
The decision to emphasize spatial or temporal resolution should be based on the pertinent clinical question to be answered.
For example,
a study to evaluate renal artery stenosis should focus more on spatial resolution.
TR-MRA does not require accurate determination of contrast bolus arrival time: the MR technologist simply starts the TR-MRA sequence and runs it until the contrast bolus has passed through the vascular bed of interest.
A much smaller doses of contrast can be used with TR-MRA than with conventional bolus-chase 3D MRA.
Conventional bolus-chase 3D MRA can be adversely affected by variability in contrast arrival times between patients and even between the extremities in one patient.
Variability in contrast arrival times can arise from poor cardiac output,
proximal stenosis,
or a pathologic condition that affects only one limb.
Venous contamination also occurs more often with bolus-chase 3D MRA due to altered cardiac status or a pathologic conditions affecting one limb,
such as cellulitis.
TR-MRA overcomes these limitations by providing quasi-real time fluoroscopic visualization of the targeted vascular bed.
For these reasons,
TR-MRA is especially well suited to image the calf and foot arteries in patients with extensive inflow disease.
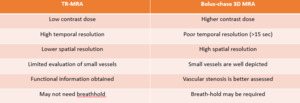
Fig. 1: Differences between TR-MRA and conventional contrast-enhanced MRA
Clinical utility of TR-MRA by anatomical region:
TR-MRA is the technique of choice for evaluation of (1) high flow vascular beds such as the carotid and renal arteries and the cardiopulmonary system,
(2) sites of unpredictable contrast arrival time,
such as the extremities in patients with peripheral vascular disease,
(3) arteriovenous malformations,
and (4) collateral and retrograde flow at sites of vascular stenoses.
The high temporal resolution of TR-MRA provides important dynamic information for detailed evaluation of arteriovenous fistula,
including feeding arteries and early draining veins.
Head and Neck:
- Evaluation of arteriovenous malformation (AVM): TR-MRA can help to identify the arterial supply,
the size and location of the AVM nidus,
and the number and type of draining veins.
A standard MRI can also be performed during the same session to provide detailed anatomy.
- Supra-aortic arteries: TR-MRA can provide hemodynamic information to evaluate atherosclerotic disease of the supraaortic arteries without venous contamination.
However,
the limited spatial resolution of TR-MRA creates a bias toward overestimation of vascular stenoses compared with high-resolution single phase contrast-enhanced 3D MRA.
Thorax
Time-resolved MRA is particularly important in thoracic imaging because it eliminates the need for long breath-holds,
which may not be possible in uncooperative,
debilitated,
or conscious sedated patients.
- Intracardiac shunts
- Patency of cardiopulmonary conduits
- Baffle leak

Fig. 2: 20 year-old female with a history of D-transposition of the great arteries repaired with Mustard procedure at one year of age. Time-resolved contrast-enhanced magnetic resonance angiography (TRICKS) was performed with 0.07mmol/kg of gadobenate dimeglumine. Time-resolved CE-MRA was used to optimize evaluation of the pulmonary arteries (C) and aorta (E) in patients with complex congenital heart disease. Abbreviations: Ao – aorta; LV – left ventricle; MPA – main pulmonary artery; RV – right ventricle.
References: University of Wisconsin
- Aortic dissection: Improved depiction of false and true lumina
- Aortic aneurysm
- Aortic stenosis: dynamic collateral flow may be seen

Fig. 3: 65 year-old male with descending thoracic aorta dissection, starting just distal to the left subclavian artery origin. Time-resolved contrast-enhanced magnetic resonance angiography (TRICKS) was performed with 0.1 mmol/kg of gadobenate dimeglumine. Time-resolved CE-MRA helps differentiate the true and false lumens.
References: University of Wisconsin

Fig. 4: 65 year-old male with descending thoracic aorta dissection, starting just distal to the left subclavian artery origin (arrow). Time-resolved contrast-enhanced magnetic resonance angiography (TRICKS) was performed with 0.1 mmol/kg of gadobenate dimeglumine. Time-resolved CE-MRA helps differentiate the true (TL) and false (FL) lumens.
References: University of Wisconsin

Fig. 5: 86 year-old male with type II endoleak afer endovascular abdominal aortic aneurysm repair. Time-resolved contrast-enhanced magnetic resonance angiography (TRICKS) was performed with 0.1 mmol/kg of gadobenate dimeglumine. Time-resolved CE-MRA helps confirm the source of the endoleak, in this case a lumbar artery (arrows).
References: University of Wisconsin
- Pulmonary vessels: TR-MRA can provide a three phase evaluation of the pulmonary vasculature,
which can be reconstructed in any plane owing to the volumetric dataset.
Concomitant angiographic and perfusion imaging can also be obtained with qualitative and/or semiquantitative evaluation of lung perfusion.
TR-MRA and perfusion imaging can be helpful in the diagnosis of pulmonary hypertension due to chronic thromboembolic disease.
The occluded artery and affected pulmonary parenchyma can be evaluated concurrently.
- Central Veins: TR-MRA provides robust mapping of central thoracic veins and facilitates detection of stenoses,
vascular anomalies and collateral flow to better define hemodynamic significance and chronicity.
- Vascular thoracic outlet syndrome.
Abdomen and Pelvis:
TR-MRA provides anatomic and dynamic evaluation of native and transplanted abdominal and pelvic organs and their vasculature.
TR-MRA rivals DSA and ultrasound for evaluating patients with suspected pelvic congestion syndrome because it directly visualizes reflux into the left ovarian vein.
TR-MRA rivals ultrasound for diagnosing uterine AVM and defining the feeding arteries and draining veins,
but lacks the superior spatial resolution of conventional angiography.

Fig. 6: Coronal MIP cine loop from contrast-enhanced time-resolved 3D MRA shows early filling of a uterine AVM involving the myometrium and endometrium. The AVM is fed by arterial supply from the anterior division of the right internal iliac artery.

Fig. 7: Oblique coronal MIP contrast enhanced TR-MRA showing early filling of uterine AVM involving the myometrium and endometrium. The AVM is fed by arterial supply from the anterior division of the right internal iliac artery.

Fig. 8: Coronal MIP cine loop from contrast-enhanced time-resolved 3D MRA shows early retrograde filling of a markedly dilated and tortuous left ovarian vein in a different patient with subsequent filling of periuterine varices.
Extremities:
TR-MRA can evaluate congenital and posttraumatic vascular malformations of the upper and lower extremities and define vascular anatomy for surgical planning.
- Thoracic outlet syndrome
- Raynaud’s disease: can be evaluated with provocative testing at multiple temperatures

Fig. 9: 44 year-old male with left upper extremity iatrogenic arteriovenous fistula (AVF). Time-resolved contrast-enhanced magnetic resonance angiography (TRICKS) was performed with 0.1 mmol/kg of gadodiamide. In patients with vascular malformations, high temporal resolution acquisitions are necessary to differentiate high-flow vascular malformations from slow-flow vascular malformations. In this patient with AVF, there is almost simultaneous enhancement of the arteries (A) and veins (V), consistent with a high-flow malformation.
References: University of Wisconsin

Fig. 10: Coronal MIP cine loop from contrast-enhanced time-resolved 3D MRA shows focal stenosis of the right subclavian artery with the right arm raised overhead (A).

Fig. 11: The stenosis resolves with the right arm down (B)
- Popliteal artery entrapment syndrome: obviates the need for contrast bolus timing. Also,
the low contrast dose for TR-MRA enables multiple contrast injections to be performed with the foot in various positions.
- Preoperative anatomic evaluation of the fibular artery and normal anterior and posterior flow into the foot before harvesting fibular bone grafts for reconstructive surgery.

Fig. 12: 45 year-old male with right lower extremity claudication due to popliteal entrapment (arrows). Time-resolved contrast-enhanced magnetic resonance angiography (TRICKS) was performed with 0.1 mmol/kg of gadobenate dimeglumine with the patient performing plantar flexion against resistance. Time-resolved CE-MRA ensures optimization of arterial phase acquisition without venous contamination.
References: University of Wisconsin

Fig. 13: Another case example of popliteal artery entrapment syndrome. Coronal MIP images from a contrast-enhanced TR-MRA show occlusion of the right popliteal artery and areas of focal stenoses in the left popliteal artery with plantar flexion

Fig. 14: 19 year-old male with left lower extremity congenital vascular malformation (arrows). Time-resolved contrast-enhanced magnetic resonance angiography (TRICKS) was performed with 0.1 mmol/kg of gadobenate dimeglumine. In patients with vascular malformations, high temporal resolution acquisitions are necessary to differentiate high-flow vascular malformations from slow-flow vascular malformations and to identify feeding arteries and draining veins.
References: University of Wisconsin


 was performed with 0.07mmol/kg of gadobenate dimeglumine. Time-resolved CE-MRA was used to optimize evaluation of the pulmonary arteries (C) and aorta (E) in patients with complex congenital heart disease. Abbreviations: Ao – aorta; LV – left ventricle; MPA – main pulmonary artery; RV – right ventricle. References: University of Wisconsin")
 was performed with 0.1 mmol/kg of gadobenate dimeglumine. Time-resolved CE-MRA helps differentiate the true and false lumens. References: University of Wisconsin")
. Time-resolved contrast-enhanced magnetic resonance angiography (TRICKS) was performed with 0.1 mmol/kg of gadobenate dimeglumine. Time-resolved CE-MRA helps differentiate the true (TL) and false (FL) lumens. References: University of Wisconsin")
 was performed with 0.1 mmol/kg of gadobenate dimeglumine. Time-resolved CE-MRA helps confirm the source of the endoleak, in this case a lumbar artery (arrows). References: University of Wisconsin")



. Time-resolved contrast-enhanced magnetic resonance angiography (TRICKS) was performed with 0.1 mmol/kg of gadodiamide. In patients with vascular malformations, high temporal resolution acquisitions are necessary to differentiate high-flow vascular malformations from slow-flow vascular malformations. In this patient with AVF, there is almost simultaneous enhancement of the arteries (A) and veins (V), consistent with a high-flow malformation. References: University of Wisconsin")
.")
")
. Time-resolved contrast-enhanced magnetic resonance angiography (TRICKS) was performed with 0.1 mmol/kg of gadobenate dimeglumine with the patient performing plantar flexion against resistance. Time-resolved CE-MRA ensures optimization of arterial phase acquisition without venous contamination. References: University of Wisconsin")

. Time-resolved contrast-enhanced magnetic resonance angiography (TRICKS) was performed with 0.1 mmol/kg of gadobenate dimeglumine. In patients with vascular malformations, high temporal resolution acquisitions are necessary to differentiate high-flow vascular malformations from slow-flow vascular malformations and to identify feeding arteries and draining veins. References: University of Wisconsin")